To be sold on retail on prescription of a Registered Medical Practitioner only.
Prescribing Information
1.0 Generic Name
Ursodeoxycholic Acid Oral Suspension
2.0 Qualitative and Quantitative Composition
Each 5ml contains: Ursodeoxycholic acid I.P. …………125 mg
In a Flavoured Sorbitol base…………………………. q.s.
Colours: Sunset Yellow FCF
3.0 Dosage Form and Strength
Dosage form: oral suspension,
Strength: 125mg/5ml
4.0 Clinical Particulars
4.1 Therapeutic Indications
For the treatment of patients with chronic cholestatic liver disease.
4.2 Posology and Method of Administration
There are no age restrictions on the use of ursodeoxycholic acid in the treatment of PBC and for the dissolution of radiolucent gallstones. The following daily dose is recommended for the various indications:
For the treatment of primary biliary cholangitis (PBC)
The daily dose depends on body weight and is approximately 14 ± 2 mg UDCA per kg of body weight.
For the first 3 months of treatment, this medicinal product should be taken divided over the day. When the liver function parameters improve, the daily dose can be administered once a day in the evening.
Body weight (kg)
Daily dose (mg/kg BW)
Amount of Suspension (ml)*
First 3 months
Subsequently –
Morning
Midday
Evening
Evening (1× daily)
8–11
12–16
–
2.5 ml
2.5 ml
5 ml
12–15
12–16
2.5 ml
2.5 ml
2.5 ml
7.5 ml
16–19
13–16
5 ml
–
5 ml
10 ml
20–23
13–15
2.5 ml
5 ml
5 ml
12.5 ml
24–27
13–16
5 ml
5 ml
5 ml
15 ml
28–31
14–16
2.5 ml
5 ml
10 ml
17.5 ml
32–39
12–16
5 ml
5 ml
10 ml
20 ml
40–47
13–16
5 ml
10 ml
10 ml
25 ml
This medicinal product should be taken in accordance with the dosage regimen given above. The oral suspension must be taken regularly.
The use of ursodeoxycholic acid in PBC may be continued indefinitely.
For dissolution of cholesterol gallstones:
Approximately 10 mg of UDCA per kg of body weight daily, equivalent to:
Body Weight (kg)
Amount of Suspension (ml)
5–7
2.5 ml
8–12
5 ml
13–18
7.5 ml
19–25
10 ml
26–35
15 ml
36–50
20 ml
The suspension should be taken in the evening at bedtime. The oral suspension must be taken regularly.
The time required for dissolution of gallstones is likely to range from 6 to 24 months depending on stone size and composition.
Follow-up cholecystograms or ultrasound investigation may be useful at 6 month intervals until the gallstones have disappeared.
Treatment should be continued until 2 successive cholecystograms and/or ultrasound investigations 4-12 weeks apart have failed to demonstrate gallstones.
Paediatric population
Cholesterol rich gallstones and PBC are very rare in children but when they occur, dosage should be related to bodyweight. There are no adequate data on the efficacy and safety in this population
Hepatobiliary disorders associated with cystic fibrosis
Paediatric population
Children with cystic fibrosis aged 1 month to 18 years: 20 mg/kg/day in 2-3 divided doses, with a further increase to 30 mg/kg/day if necessary. Very rarely, children under 10 kg body weight are affected. In this case, a commercially available oral syringe should be used. Please note: a syringe is not provided in the pack.
Up to 10 kg body weight: Dosing 20 mg UDCA/kg/day
More than 10 kg body weight (BW): Dosing 20-25 mg UDCA/kg/day
4.3 Contraindications
Ursodeoxycholic acid tablets should not be used in patients with:
Acute inflammation of the gall bladder or bile ducts.
Occlusion of the biliary tract (occlusion of the common bile duct or a cystic duct).
Frequent episodes of biliary colic.
X-ray radiolucent calcified gallstones.
Impaired contractility of the gallbladder.
Hypersensitivity to bile acids or to any of the excipients.
Active gastric and duodenal ulcers.
Paediatric population
Unsuccessful portoenterostomy or without recovery of good bile flow in children with biliary atresia.
4.4 Special Warnings and Precautions for use
Ursodeoxycholic acid tablets should be taken under medical supervision.
During the first three months of the treatment liver function parameters AST (SGOT), ALT (SGPT) and γ-GT should be monitored by the physician every 4 weeks, thereafter every 3 months. Apart from allowing for identification of responders and non-responders in patients being treated for primary biliary cholangitis, this monitoring would also enable an early detection of potential hepatic deterioration, particularly in patients with advanced primary biliary cholangitis.
When used for dissolving gallstones:
In order to be able to assess the therapeutic progression of the dissolution of gallstones and to timely identify a possible calcification of the stones, the gall bladder, depending on the size of the stones, should be visualized 6 to 10 months after the start of the treatment (oral cholecystography) with total image and occlusions and in the standing and lying position (ultrasound investigation).
If the gallbladder cannot be visualized on X-rays, or in cases of calcified gallstones, impaired contractility of the gall bladder or frequent episodes of biliary colic, the treatment with Ursodeoxycholic acid should be discontinued.
When used for the treatment of advanced primary biliary cholangitis:
In very rare cases decompensation of liver cirrhosis is observed which partially decreased after treatment discontinuation.
In patients with PBC, the clinical symptoms may worsen in rare cases at the start of treatment, e.g. pruritus may increase. In this case, the therapy is to be continued with a dose reduction and subsequently should be gradually increased to the recommended dose.
If diarrhoea occurs, the dosage should be reduced, and treatment should be discontinued in case of persistent diarrhoea.
Female patients who use Ursodeoxycholic acid for dissolving gall stones must use an effective non-hormonal method of contraception, since hormonal contraception may increase biliary lithiasis
4.5 Drug Interactions
Ursodeoxycholic acid tablets should not be used concurrently with colestyramine, colestipol, or an antacid, on the basis of aluminium hydroxide and/or smectite (aluminium oxide), because these preparations bind ursodeoxycholic acid in the intestine and thereby inhibits its absorption and efficacy. If the use of such a medicine is necessary, must it be taken at least 2 hours before or after Ursodeoxycholic acid.
Ursodeoxycholic acid may affect the absorption of ciclosporin from the intestine. In patients treated with ciclosporin the blood level of ciclosporin should be monitored and the ciclosporin dose should be adjusted, if necessary.
In isolated cases Ursodeoxycholic acid can reduce the absorption of ciprofloxacin.
In a clinical study in healthy volunteers, the concomitant use of UDCA (500 mg/day) and rosuvastatin (20 mg/day) resulted in slightly elevated plasma levels of rosuvastatin. The clinical relevance of this interaction, also with other statins, is not known. Ursodeoxycholic acid has been shown to reduce the peak plasma concentration (Cmax) and the AUC of the calcium antagonist nitrendipine in healthy volunteers. Close monitoring of the outcome of concurrent use of nitrendipine and ursodeoxycholic acid is recommended. An increase of the dose of nitrendipine may be necessary. An interaction with a reduction of the therapeutic effect of dapsone was also reported. These observations, together with in vitro findings could be an indication that ursodeoxycholic acid can induce cytochrome P450 3A enzymes. Induction has, however not been observed in a well-designed interaction study with budesonide, which is a known cytochrome P450 3A substrate.
Oestrogens and blood cholesterol lowering agents such as clofibrate increase hepatic cholesterol secretion and may therefore encourage biliary lithiasis; which is a counter-effect to ursodeoxycholic acid used for dissolution of gallstones
4.6 Use in special populations
Pregnancy
There are no or limited amount of data from the use of ursodeoxycholic acid in pregnant women. Studies in animals have shown reproductive toxicity during the early gestation phase
Women of childbearing potential
Women of childbearing potential should be treated with ursodeoxycholic acid, only if they practice reliable contraception: non-hormonal contraceptives or oral contraceptives with low oestrogen dose are recommended. However, in patients taking Ursodeoxycholic acid for dissolving gallstones an effective non-hormonal contraception should be used, since hormonal oral contraceptives may increase biliary lithiasis. The possibility of a pregnancy must be excluded before beginning treatment.
Breastfeeding
According to few documented cases of breastfeeding women milk levels of ursodeoxycholic acid levels in milk are very low and probably no adverse reactions are to be expected in breastfed infants.
Lactation
Cetirizine, the racemate of levocetirizine, has been shown to be excreted in human milk. Therefore, the excretion of levocetirizine in human milk is likely. Adverse reactions associated with levocetirizine may be observed in breastfed infants. Therefore, caution should be exercised when prescribing levocetirizine to lactating women.
Fertility
Animal studies did not show an influence of ursodeoxycholic acid on fertility. Human data on fertility treatment with ursodeoxycholic acid are not available.
4.7 Effects on Ability to Drive and Use Machines
Ursodeoxycholic acid has no or negligible influence on the ability to drive and use machines.
4.8 Undesirable Effects
The following adverse reactions have been reported during clinical trials and are ranked using the following frequency: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to 1/1,000); very rare (<1/10,000); not known (cannot be estimated from the available data).
Gastrointestinal disorders:
In clinical studies, reports of pasty stools or diarrhoea during treatment with ursodeoxycholic acid were common. In very rare cases, severe right upper abdominal pain has occurred during the treatment of primary biliary cholangitis.
Hepatobiliary disorders:
During treatment with ursodeoxycholic acid calcification of gallstones can occur in very rare cases. During the treatment of advanced stages of primary biliary cholangitis decompensation of cirrhosis has been observed in very rare cases, which partially regressed after treatment discontinuation.
Hypersensitivity reactions:
Very rarely urticaria may occur.
Reporting of Suspected Adverse Reactions
Reporting suspected adverse reactions after authorization of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via email to: medico@zorvia.com
By reporting side effects, you can help provide more information on the safety of this medicine.
4.9 Overdose
In the case of overdose diarrhoea may occur. In general, other symptoms of overdose are unlikely, because the absorption of the ursodeoxycholic acid decreases with increasing dose and therefore more is excreted in the faeces.
If diarrhoea occurs, the dosage should be reduced, and treatment should be discontinued in case of persistent diarrhoea.
No specific measures are needed and the consequences of diarrhoea should be treated symptomatically with restoration of fluid and electrolyte balance.
Additional information or special populations
Long-term, high-dose UDCA therapy (28-30 mg/kg/day) by patients with primary sclerosing cholangitis (off-label use) was associated with a higher frequency of serious adverse events.
5.0 Pharmacological Properties
5.1 Mechanism of action
Ursodeoxycholic acid, a naturally occurring bile acid found in small quantities in normal human bile and in the bile of certain other mammals. It suppresses hepatic synthesis and secretion of cholesterol, and also inhibits intestinal absorption of cholesterol.
5.2 Pharmacodynamic properties
Bile acids are among the most important components of the bile and play a role in the stimulation of bile secretion. Bile acids are also important to keep the cholesterol in bile in solution. In a healthy person, the ratio between the concentration of cholesterol and bile acids in the bile is such that the cholesterol will remain in solution for most of the day. In this case, no gallstones can form (the bile is non-lithogenic). In patients with cholesterol stones in the bile, this ratio is changed, and the bile is supersaturated with cholesterol (bile is lithogenic). This may cause a precipitation of cholesterol crystals and the formation of gallstones after some time.
The ursodeoxycholic acid converts lithogenic bile in non-lithogenic bile and gradually dissolves the cholesterol gallstones.
Investigations of the effect of ursodeoxycholic acid on the cholestasis in patients with impaired biliary drainage and on the clinical symptoms in patients with primary biliary cholangitis and cystic fibrosis have shown that cholestatic symptoms in the blood (to be measured by the increased value of alkaline phosphatase (AF), gamma- GT and bilirubin) and the itch declined rapidly, while also the fatigue decreased in the majority of patients. Moreover, studies seem to indicate a positive benefit-risk ratio of the ursodeoxycholic acid in children and young adult cystic fibrosis patients with mild to moderate hepatobiliary disorders.
Paediatric population
Cystic fibrosis
From clinical reports long-term experience of 10 years and more has been gained with UDCA therapy in paediatric patients suffering from cystic fibrosis associated hepatobiliary disorders (CFAHD). There is evidence that treatment with UDCA can inhibit bile duct proliferation, can halt progression of histological damage and even reverse hepato-biliary changes, if it happens at an early stage of CFAHD. The treatment with UDCA should be started as soon as the CFAHD diagnosis is made, in order to optimize the effectiveness of the treatment.
5.3 Pharmacokinetic properties
About 90% of the therapeutic dose of the ursodeoxycholic acid is rapidly absorbed in the small intestine after oral administration.
After the absorption, ursodeoxycholic acid is absorbed in the liver (there is a substantial "first pass-effect"), where it is conjugated with glycine or taurine and then secreted into the bile ducts. Only a small portion of ursodeoxycholic acid is found in the systemic circulation. This is excreted renally. With the exception of conjugation, ursodeoxycholic acid is not metabolised. However, a small fraction of orally administered ursodeoxycholic acid undergoes bacterial conversion to 7-keto- lithocholic acid resp. lithocholic acid after each enterohepatic circulation, while bacterial deconjugation also takes place in the duodenum. Ursodeoxycholic acid, 7- keto-lithocholic acid and lithocholic acid are relatively poorly soluble in water, so a large part of it is excreted via the bile into the faeces. Resorbed ursodeoxycholic acid is conjugated again by the liver; 80% of the lithocholic acid formed in the duodenum is excreted in the faeces, but the remaining 20% of it are sulphated by the liver to insoluble lithocholyl conjugates after absorption, which in turn are excreted via the bile and faeces.
Resorbed 7-keto-lithocholic acid is reduced to chenodeoxycholic acid in the liver.
Lithocholic acid can cause cholestatic liver damage, when the liver is unable to sulphate the lithocholic acid. Although a reduced capacity to sulphate the lithocholic acid in the liver is found in some patients, there is for the time being no clinical evidence that cholestatic liver damage can be associated with the therapy using ursodeoxycholic acid.
After repeated dosage, the ursodeoxycholic acid concentration in the bile reaches a "steady state" after approximately 3 weeks: the total concentration of the ursodeoxycholic acid, however, is never higher than about 60% of the total concentration of the bile acid in the bile: also, at high doses.
After therapy with ursodeoxycholic acid is stopped, the concentration of ursodeoxycholic acid in bile decreases quickly after 1 week to 5-10% of the "steady- state" concentration.
The biological half-life of ursodeoxycholic acid is approximately 3.5 to 5.8 days.
6.0 Nonclinical Properties
6.1 Animal Toxicology or Pharmacology
Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicity, genotoxicity, carcinogenic potential, toxicity to reproduction.
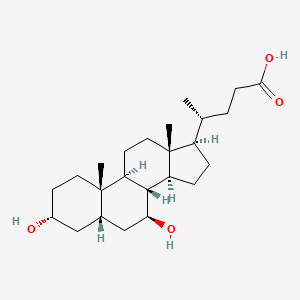
7.0 Description
Ursodeoxycholic acid is 3α,7β-Dihydroxy-5β-cholan24-oic acid. The empirical formula is C24H40O4 and its molecular wight is 392.6 g/mol. The chemical structural formula is:
structural formula
8. Pharmaceutical particulars
8.1 Incompatibilities
Not applicable
8.2 Shelf-Life:
Refer on pack
8.3 Packaging Information:
60ml & 100ml Bottle
8.4 Storage and Handling Instructions
Store below 300C. Protect from light.
9.0 Patient Counselling Information
Ask the patients to inform the treating physicians in case of any of the below:
Have any allergies.
Have kidney or liver problems.
Are pregnant or plan to become pregnant.
Are breastfeeding or plan to breastfeed.
Have any serious illness.
Are taking any medicines (prescription, over the counter, vitamins, or herbal products)